What is Radiation?
Radiation is a fundamental phenomenon that exists as a natural part of the world and universe. It is the emission and propagation of energy in the form of waves or particles through space or a material medium. At its most basic level, radiation occurs when unstable atomic nuclei release energy by emitting particles (such as alpha particles, beta particles, or neutrons) and/or electromagnetic waves (such as gamma rays). Electromagnetic radiation is also produced through several other processes: X-rays are generated when electrons transition between inner atomic energy levels or when fast-moving electrons are decelerated (bremsstrahlung), while UV radiation primarily comes from electron transitions in excited gases and thermal emission from very hot objects such as the sun. The impact of radiation has the potential to be either beneficial or destructive to biological systems.
Ionizing and Non-ionizing Radiation
Radiation is categorizable into two groups: ionizing radiation and non-ionizing radiation. Ionizing radiation has enough energy to remove tightly bound electrons from atoms, creating charged particles (ions). This group includes alpha particles, beta particles, gamma rays, X-rays, and neutrons. Ionizing radiation is commonly associated with medical applications, such as X-rays and radiotherapy, but it also occurs naturally, as in the form of cosmic rays or radon decay.
In contrast, non-ionizing radiation does not have sufficient energy to ionize atoms or molecules. This group includes ultraviolet (UV) radiation, visible light, infrared radiation, microwaves, and radio waves. However, ultraviolet (UV) radiation exists on the boundary: lower-energy UV radiation is typically non-ionizing, while higher-energy UV radiation, such as extreme UV, can ionize atoms and molecules. Non-ionizing radiation is generally less harmful and technologies such as communication devices and heating systems use it. On the beneficial side, the visible light radiation coming from the sun enables photosynthesis in plants and infrared radiation provides warmth. As is also common knowledge, the use of X-Rays in medicine is very popular in current times.
Regardless of whether radiation is produced naturally through something such as UV rays, or the high-energy radiation created by humans for radiotherapy and other medical procedures, there are biological impacts for any living creature that encounters it. Today, we will explore the impact of radiation on a cellular level and why, despite these potentially harmful effects, the risk is worth the reward when it comes to continued radiation use.
How Does it Affect the Body Overall?
Ionizing radiation can cause damage to one’s cells in different ways:
- Direct DNA Damage: Ionizing radiation directly strikes the DNA, which breaks chemical bonds and causes mutations in the genetic code1.
- Indirect Cellular Damage: The radiation may ionize water molecules within the body, which creates highly reactive “free radicals”. These free radicals are then capable of damaging cellular components, which can include DNA, proteins, and lipids.2
Cellular Impact of Radiation
Although any cell within the body exposed to ionizing radiation can have a reaction to it, the impact of this radiation depends heavily on which types of cells are exposed and the intensity of the radiation. Cells, by default, have mechanisms to repair DNA damage. Should the repair be successful, then the cell can continue to function as normal.
Some of the human body’s cells, especially those that have rapidly dividing tissues such as bone marrow and the gastrointestinal system, are more vulnerable to radiation damage.3
Animal Cells and Irradiation Effects
- DNA Damage and Mutations: Damage to DNA is probably the most significant consequence of radiation exposure. Radiation can cause single-strand or double-strand breaks in the DNA, which may lead to mutations or chromosomal abnormalities as a result of errors in the repair process. Any such DNA mutation can alter how genes normally function and may result in cancerous growths or even developmental abnormalities, should the cell replicate with damaged DNA.4
- Cell Death: Most commonly, cell death from radiation is mitotic death. During the process of cell division, damage to the chromosomes cause cells to fail to complete their replication and die. This occurs most often when radiation damage is severe enough, as happens with double strand breaks, causing failed or incorrect repair. A secondary type of cell death that may occur is apoptosis. Apoptosis, known as programmed cell death, is normally a natural process to aid in getting rid of dysfunctional or no longer needed cells. For example, apoptosis is what allows the tadpole to lose its tail. Radiation damage may also cause a cell to enter into the apoptosis cycle leading to cell death and impaired organ function.5 Radiation induced apoptosis, however, is highly dependent on the type of cell being most common blood cells and cells associated with the immune system.
- Genetic Instability and Cancer: One of the most concerning effects of radiation on cells is the potential to cause cancer. The DNA mutations mentioned earlier can lead to the development of oncogenes (genes that promote cancer) or the inactivation of tumor suppressor genes. When these changes happen in critical genes that control the cell cycle and cell division, it can result in uncontrolled cell growth. This, more often than not, leads to cancer.5
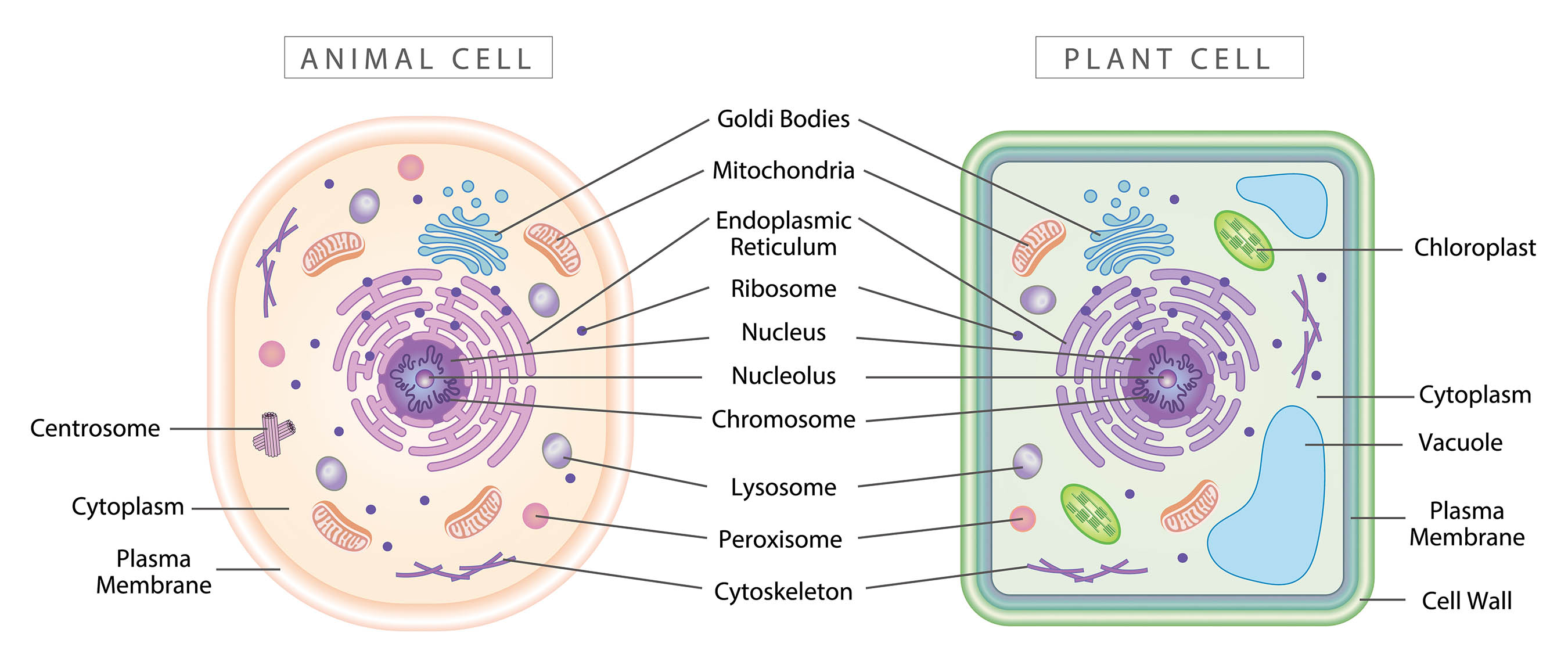
Plant cells also may suffer radiation damage. Due to differences of structure and metabolism between animal and plant cell types, plant cells have a higher resistance to the effects of radiation making them more tolerant to ionizing radiation than animals.6 For plants, radiation has a less significant impact and can sometimes produce beneficial effects.
Plant Cells and Irradiation Effects
- DNA Damage and Mutations: As with animal cells, the nucleus of plant cells is the area of highest injury from ionizing radiation. The amount of damage that may occur to the DNA is dependent on chromosome volume. This volume changes between plants and is also affected by the different stages of the plant life cycle. Mutations (DNA deletions, base substitutions, and chromosomal alterations) can vary from non-lethal to lethal depending on the dosage of radiation exposure. 6
- Phenotypical Responses: As a consequence of the genetic mutations plant cells may develop after radiation exposure, the plant itself can go through a phenotypical response such as reduced growth, altered leaf morphology, and impaired development. High doses of irradiation (several Gy) can likely cause structural modifications during the plant’s growth, but chronic low levels of radiation may also introduce changes in plant traits. These studies are normally done with plant seeds that are irradiated and then observed as they develop. However, if the exposed cells have greater radioresistance, this resistance will prevent them from producing a more pronounced phenotypical response as the seed matures.6
- Photosynthesis: High doses of gamma radiation exposure to plants can result in a decrease of photosynthesis by disrupting the photosynthetic pigment–chlorophyll–and the photosynthetic electron transfer rate in some plants. As with the potential for DNA damage or mutations however, the impact to photosynthesis can be influenced by the plant’s developmental stage with younger or actively growing plants potentially experiencing a more significant impact compared to mature plants.6
How Radiation can Beneficially Impact the Body
Despite the tendency to associate the aforementioned biological effects with harm, radiation can have positive applications. These are mostly within the medical field but are recognizable throughout other industries as well. Here are a few ways that humans have turned the potency of radiation into a benefit:
Cancer Treatment (Radiotherapy):
Cancer treatment is, unsurprisingly, one of the most significant uses of radiation for good. High-energy radiation is usable for targeting and destroying cancerous cells by decreasing the rate of tumor cell proliferation through cell cycle arrest stimulated by DNA damage. By preferentially focusing radiation on solid tumors and limiting the dose to normal critical structure, cancer cells may be either killed or shrunk sufficiently to prevent cancer from spreading or to make it easier to remove through other means. Cancer cells divide rapidly, which makes them more sensitive to radiation than normal cells making them an ideal target for radiation therapy.7
- Radiation in Chemotherapy: Radiation therapy is usable in conjunction with chemotherapy drugs, which increases the effectiveness of an overall treatment plan and can prevent tumor growth.8
- Precision Medicine: This method was designed to help healthcare providers deliver more personalized treatments. In cancer care, it considers how variations in specific genes or proteins in a patient’s cancer cells may influence treatment choices. Radiation can benefit cancer treatment specifically through precision medicine when using targeted therapy that includes radiopharmaceuticals.9 An example of a targeted therapy is one that uses antibodies to which a radioactive atom has been attached. The antibody recognizes particular antigens expressed by tumor cells and bind to the cell thereby delivering its radioactive package.
Medical Imaging and Diagnostics
Diagnostic work and medical imaging benefit from radiation as well, as we’ve covered in previous blogs. Whether they are imaging options such as X-rays and CT scans, or nuclear medicine diagnostics using injected radioactive tracers, these techniques allow doctors to visualize internal structures of the body. This helps with diagnosis and monitoring of various health conditions and provides detailed anatomical information needed for planning radiation therapy. Although these procedures do involve exposure to low doses of radiation, the reward of accurate diagnosis and treatment planning to manage radiation treatment in the long run is worth the small but inherent risk.
Sterilization and Disinfection
Somewhat within and outside of the medical field, sterilizing medical equipment and food products is possible with ionizing radiation. This helps to reduce the risk of foodborne illnesses and infections. This is a process known as radiation sterilization. Through it, controlled doses of radiation can help to destroy bacteria, viruses, and other pathogens.
Balancing the Positive and Negative Aspects
The impact that radiation has at the cellular level and on the overall body is a double-edged sword: the potential to heal can also be potential for harm. When using radiation for things like treatment or imaging, the difficulty lies in ensuring as small a risk as possible while maximizing the benefit. Precise and controlled radiation doses in these procedures require careful planning and monitoring that have been developed over the years.
One of the arguments for the benefits of radiation exists in a hypothesis for how radiation can impact the body depending on dosage. Despite the harmful effects of radiation that we detailed earlier, scientists have seen evidence for some beneficial effects in an area known as radiation hormesis.
The radiation hormesis model supports the idea that low-dose radiation can stimulate adaptive or protective mechanisms within cells (both plant and mammalian) when exposed. This low-dose radiation can aid with prevention of both spontaneous and toxicant-related cancers, along with other adverse health effects. Through this stimulation, the adaptive protection developed by the cells would thereby improve health.10 The radiation hormesis model, though well known by professionals in the field, requires more research, time, and development. There are no accredited organizations in the medical physics world that recognize radiation hormesis as a usable model and the LNT (Linear-No-Threshold) model maintains as the worldwide safety standard.
Conclusion
Even if human-made radiation had never come to exist, natural radiation makes it an intrinsic part of our lives. Knowing the biological impact that radiation can have down to the cellular level allows us to harness its potential in the safest ways possible for the greatest benefits and smallest risk. Although radiation can damage cells in a way that leads to mutations, cancer, or even organ failure, it is vital in treating diseases, making diagnoses, and sterilizing necessary items like food or medical equipment. As with many sources in the world, humans must strike a balance with its use. Through understanding the full effects of radiation, good and bad, we pave the way to using radiation in an effective and responsible manner.
Sources
- Ionizing Radiation and Non-Ionizing Radiation – Frequently Asked Questions a RESOURCE for VETERANS, SERVICE MEMBERS, and THEIR FAMILIES. https://www.warrelatedillness.va.gov/WARRELATEDILLNESS/education/factsheets/Radiation.pdf
- Di Meo S, Venditti P. Evolution of the Knowledge of Free Radicals and Other Oxidants. Oxidative Medicine and Cellular Longevity. 2020;2020:1-32. doi:https://doi.org/10.1155/2020/9829176
- Nuclear Regulatory Commission. Reactor Concepts Manual Biological Effects of Radiation Biological Effects of Radiation.; 2023. https://www.nrc.gov/reading-rm/basic-ref/students/for-educators/09.pdf
- Baskar R, Dai J, Wenlong N, Yeo R, Yeoh KW. Biological response of cancer cells to radiation treatment. Frontiers in Molecular Biosciences. 2014;1(24). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4429645/
- Little JB. Principal Cellular and Tissue Effects of Radiation. Nih.gov. Published 2014. https://www.ncbi.nlm.nih.gov/books/NBK12344/
- Arena C, De Micco V, Macaeva E, Quintens R. Space radiation effects on plant and mammalian cells. Acta Astronautica. 2014;104(1):419-431. doi:https://doi.org/10.1016/j.actaastro.2014.05.005
- American Cancer Society. How Radiation Therapy Is Used to Treat Cancer. www.cancer.org. Published December 27, 2019. https://www.cancer.org/cancer/managing-cancer/treatment-types/radiation/basics.html
- Rallis KS, Yau THL, Sideris M. Chemoradiotherapy in Cancer Treatment: Rationale and Clinical Applications. Anticancer Research. 2021;41(1):1-7. doi:https://doi.org/10.21873/anticanres.14746
- Xiong Y, Jian H, Han X, Li L, Zhou L. A decade of incremental advances in radiopharmaceuticals: a promising future ahead. Journal of Translational Medicine. 2024;22(1). doi:https://doi.org/10.1186/s12967-024-05891-4
- Vaiserman AM. Radiation hormesis: historical perspective and implications for low-dose cancer risk assessment. Dose Response. 2010;8(2):172-191. Published 2010 Jan 18. doi:10.2203/dose-response.09-037.Vaiserman